Accurate interpretation of gynecologic pelvic MRI depends on tailored protocols, thorough anatomic knowledge, and a systematic lesion-based approach. This review outlines classification by lesion origin and tissue composition.
MRI is used routinely in patients with gynecologic conditions due to its superior soft-tissue contrast and multiplanar capability. It can provide a detailed assessment of pelvic anatomy, lesion origin, tissue characteristics, and disease extent. Its indications include (a) characterizing US-indeterminate adnexal masses, (b) evaluating the cause of pelvic pain and abnormal uterine bleeding, © mapping symptomatic uterine leiomyomas and differentiating them from uterine sarcomas, (d) staging gynecologic cancers, and (e) addressing complex congenital müllerian duct anomalies. Additional indications include evaluating for pelvic floor dysfunction, fistulas, or placental abnormalities.
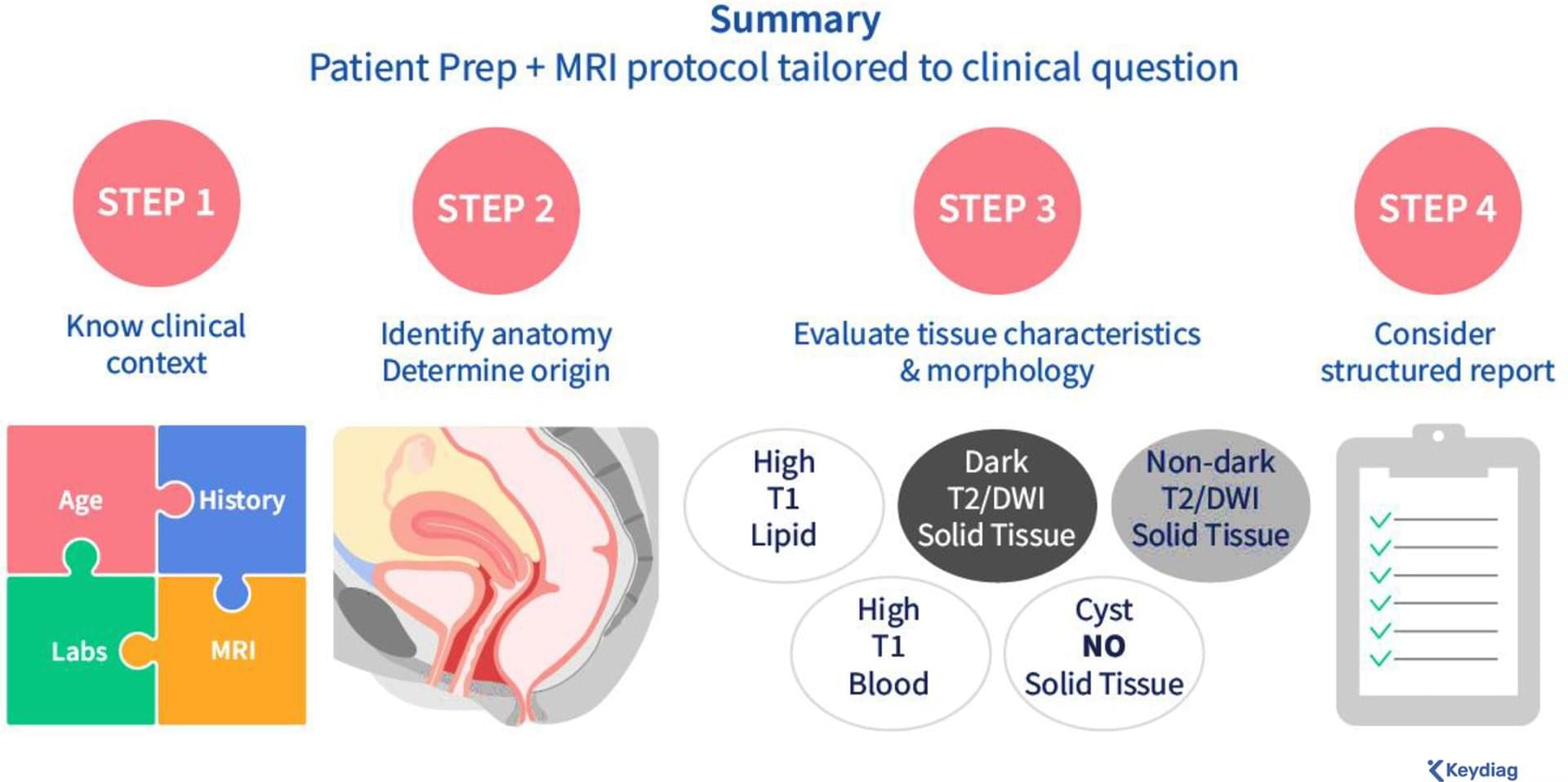
This article aims to enhance the interpretation of female pelvic MRI for gynecologic conditions. After outlining patient preparation, tailored MRI protocols, and the normal female pelvic anatomy, a step-by-step approach to interpretation is presented, focusing on evaluating lesion origin, lesion tissue composition, and solid tissue morphology (Fig 1). The review also emphasizes the importance of incorporating the patient’s clinical history to narrow the differential diagnosis and the role of disease-specific structured reporting in improving communication (Fig 1).
{kind=link}